American Diabetes Association® Releases 2018 Standards of Medical Care in Diabetes, with Notable New Recommendations for People with Cardiovascular Disease and Diabetes
Comprehensive recommendations reflect the latest advances in evidence-based research to improve care for millions of people with diabetes

ARLINGTON, Va., Dec. 8, 2017 /PRNewswire/ -- Notable new recommendations in the 2018 edition of the American Diabetes Association's (ADA's) Standards of Medical Care in Diabetes (Standards of Care) include advances in cardiovascular disease risk management including hypertension; an updated care algorithm that is patient-focused; the integration of new technology into diabetes management; and routine screening for type 2 diabetes in high-risk youth (BMI >85th percentile plus at least one additional risk factor). The Standards of Care provide the latest in comprehensive, evidence-based recommendations for the diagnosis and treatment of children and adults with type 1, type 2 or gestational diabetes, strategies to improve the prevention or delay of type 2 diabetes, and therapeutic approaches that reduce complications and positively affect health outcomes. The Standards of Care are published annually and will be available online at 4:00 p.m. ET, December 8, 2017, and as a supplement to the January 2018 print issue of Diabetes Care.

Experience the interactive Multichannel News Release here: https://www.multivu.com/players/English/8010331-american-diabetes-association-standards-of-medical-care-2018/
Beginning in 2018, the ADA will update and revise the online version of the Standards of Care throughout the year with necessary annotations if new evidence or regulatory changes merit immediate incorporation. This will ensure that the Standards of Care provide clinicians, patients, researchers, health plans and policymakers with the most up-to-date components of diabetes care, general treatment goals and tools to evaluate the quality of care. The Standards of Care will also be available as a user-friendly and interactive app for both web and mobile devices in the spring of 2018. The app will allow clinicians to access the most up-to-date information conveniently and will include interactive tools, such as a diabetes risk calculator and diabetes treatment algorithm.
"The Standards of Care are the primary resource for the optimal management of diabetes, and include updated guidelines for diabetes diagnosis, and for evidence-based prevention of diabetes and diabetes-related complications. We are especially proud of the new recommendations for patients with diabetes and cardiovascular disease," said ADA's Chief Scientific, Medical and Mission Officer William T. Cefalu, MD. "Since 1989, the American Diabetes Association has provided annual updates to the Standards of Care, and the Standards are accepted as the global standard for diabetes care. As new technology, research and treatments continue to improve and emerge, we are pleased that we will have the capacity to provide real-time updates to the Standards of Care throughout the year."
The Standards of Care incorporate comprehensive information based upon current research findings and an extensive body of literature. The important changes and updates in the 2018 edition are:
Cardiovascular disease and diabetes
- Based upon the results of multiple cardiovascular outcome trials (CVOT), there are new treatment recommendations for adults with type 2 diabetes, suggesting a pathway for people with heart disease that, after lifestyle management and metformin, should include a medication validated to improve heart health. A new table outlines the data from recent CVOT studies, and a new figure details our recommendations based on those CVOT studies. (Section 8, page S76, Table 9.4 and Figure 8.1, respectively)
- Four major, randomized controlled trials that compared intensive versus standard hypertension treatment strategies are summarized and outlined in a new table, providing support for the ADA's recommendations that most adults with diabetes and hypertension should have a target blood pressure of <140/90 mmHg and that risk-based individualization to lower targets, such as 130/80 mmHg, may be appropriate for some patients. The studies highlighted include the Action to Control Cardiovascular Risk in Diabetes Blood Pressure (ACCORD BP) trial; the Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation—Blood Pressure (ADVANCEBP) trial; the Hypertension Optimal Treatment (HOT) trial; and the Systolic Blood Pressure Intervention Trial (SPRINT). (Section 9, page S88, Table 9.1)
- A new algorithm illustrating the recommended antihypertensive treatment approach for adults with diabetes and confirmed hypertension (blood pressure ≥140/90 mmHg) has been added. (Section 9, page S90, Figure 9.1)
- Also new this year is the recommendation that all hypertensive patients with diabetes monitor their blood pressure at home to help identify potential discrepancies between office vs. home blood pressure, and to improve medication-taking behavior. (Section 9, page S87)
Screening youth for type 2 diabetes
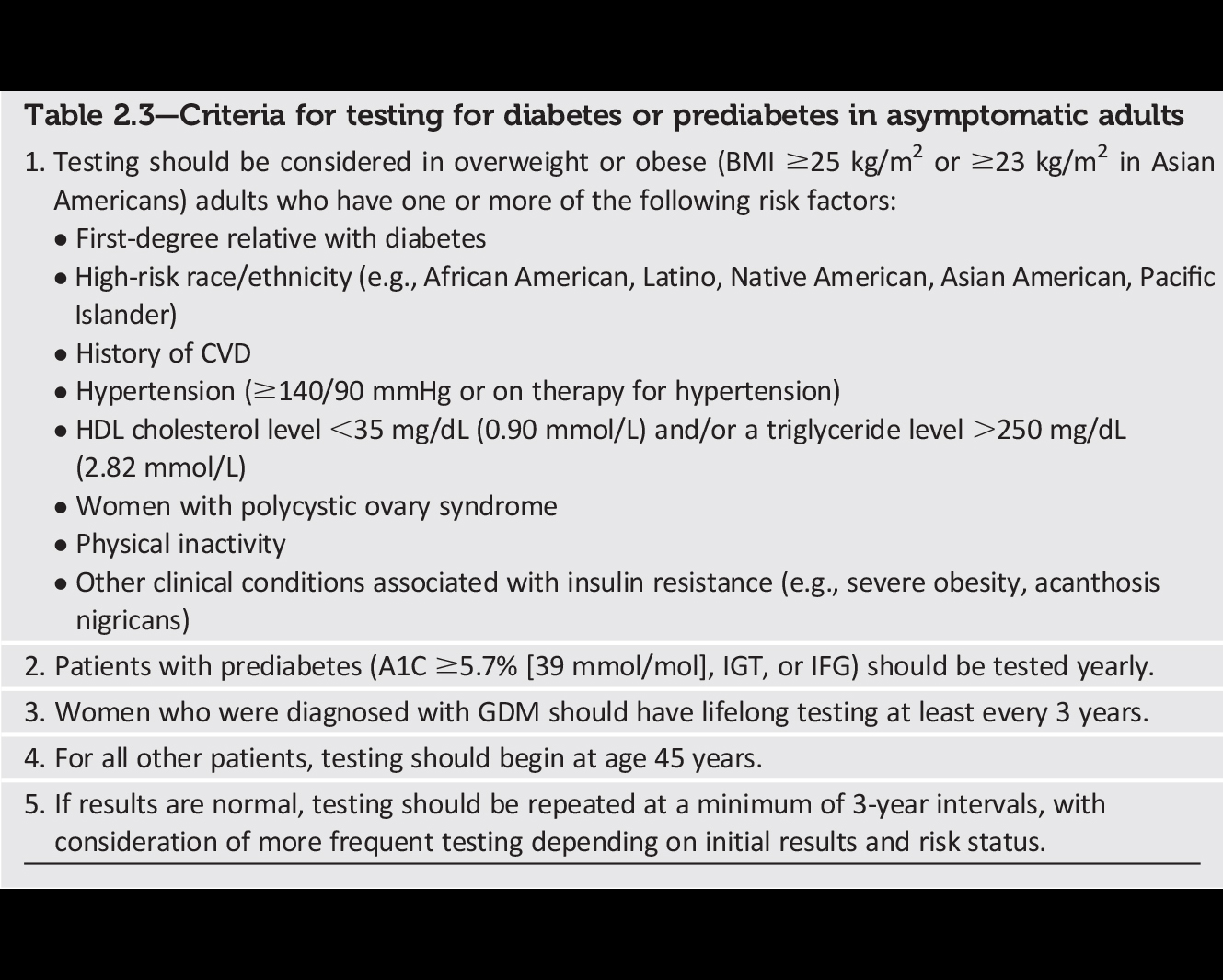
- Updated recommendations emphasize that testing for prediabetes and type 2 diabetes should be considered in children and adolescents younger than 18 years of age who are overweight or obese (BMI >85th percentile for age and sex, weight for height >85th percentile, or weight >120% of ideal for height), and have one or more additional risk factors for diabetes such as (1) maternal history of diabetes or gestational diabetes during the child's gestation; (2) family history of type 2 diabetes in first- or second-degree relative; (3) race/ethnicity (Native American, African American, Latino, Asian American, Pacific Islander; and/or (4) signs of insulin resistance or conditions associated with insulin resistance (acanthosis nigricans, hypertension, dyslipidemia, polycystic ovary syndrome, or small-for-gestational-age birth weight). (Section 2, page S19, Table 2.5)
Health technology and diabetes management
- The ADA recommends including technology-based methods, along with individual and group settings, for the delivery of effective diabetes self-management education and support. (Section 4, page S38)
- As continuous glucose monitoring (CGM) technology continues to evolve, the ADA adjusted its recommendations to align with recent data showing that CGM helps improve glycemic control for adults with type 1 diabetes starting at age 18 (previous recommendations were for those ages 25 and older). (Section 6, page S55)
- Federal regulatory changes prompted the ADA to include language describing CGM devices that don't require confirmation from finger sticks to make treatment decisions, and a new type of "flash" CGM that doesn't have any alarms and only provides "on demand" glucose readings. (Section 6, page S56)
A1C test considerations
- Additional language and recommendations have been added to help ensure appropriate use of the A1C test to diagnose diabetes and for monitoring glycemic control in people with diabetes. The A1C can give skewed results in people with certain conditions that alter the lifespan of red blood cells in the body (the ability of the A1C test to provide a measure of average blood glucose over time is based on the lifespan of red blood cells), as well as in people with certain genetic traits that alter the molecules in their red blood cells. Age, ethnicity and pregnancy can also affect A1C results. The ADA emphasizes that health care providers need to be aware of these limitations, to use the correct type of A1C test and to consider alternate diagnostic tests (fasting plasma glucose test or oral glucose tolerance test) if there is disagreement between A1C and blood glucose levels. (Section 2, page S14)
Diabetes management in specific groups
- Three new recommendations were added to highlight the importance of individualizing pharmacologic therapy for older adults with diabetes to reduce the risk of hypoglycemia, avoid overtreatment and simplify complex regimens while maintaining personalized blood glucose targets. (Section 11, page S122)
- A new guideline recommends all pregnant women with preexisting type 1 or type 2 diabetes should consider daily low-dose aspirin starting at the end of the first trimester in order to reduce the risk of pre-eclampsia. (Section 13, page S140)
Patient-centered care and acknowledging cost-of-care impact
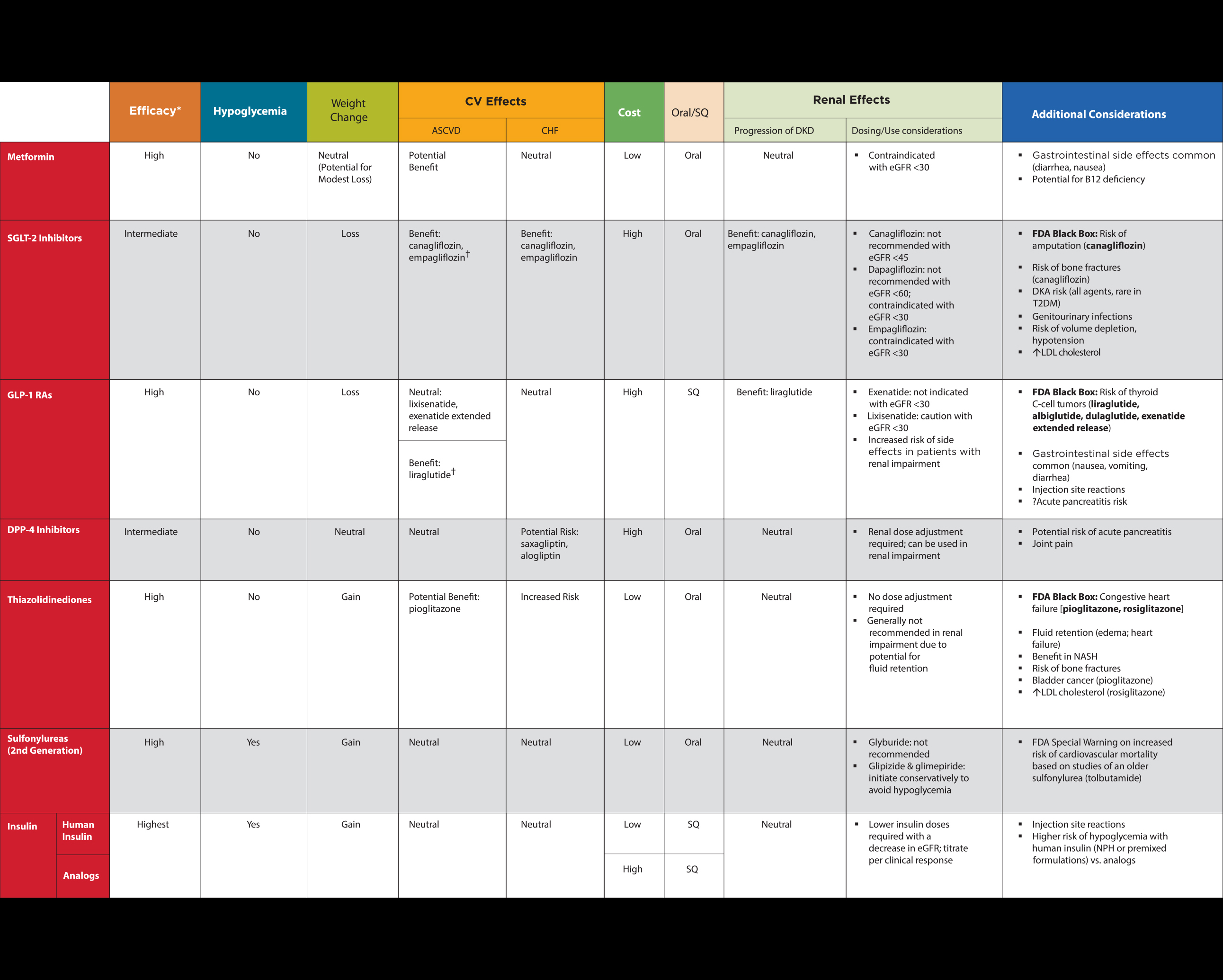
- A new table summarizes drug-specific and patient factors that may impact diabetes treatment. The chart includes the most relevant considerations, such as risk of hypoglycemia, weight effects, kidney effects and costs for all preferred diabetes medications, in one location to guide the choice of antihyperglycemic agents as part of patient-provider shared decision-making. (Section 8, page S77, Table 8.1)
- The guidelines recommend increased awareness and screening for social determinants of health such as financial ability to afford medication; access to healthy foods and food insecurity; and community support. (Section 1, page S9)
Additional important updates
- The immunization needs for people with diabetes were clarified and updated to more closely align with recommendations from the Centers for Disease Control and Prevention. (Section 3, page S29-31)
- A new section describes emerging evidence that specific glucose-lowering medications delay the onset and progression of kidney disease. (Section 10, page S108)
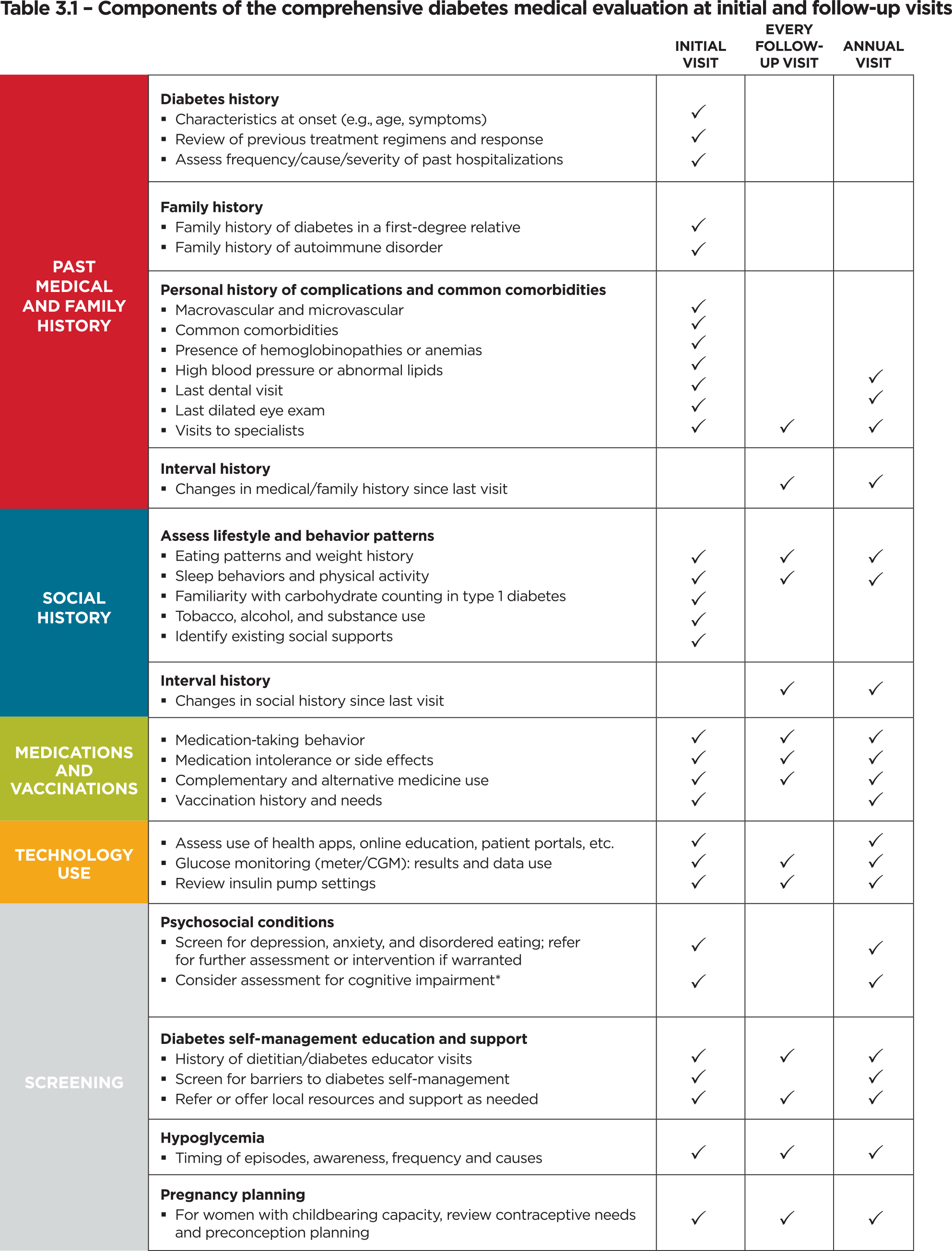
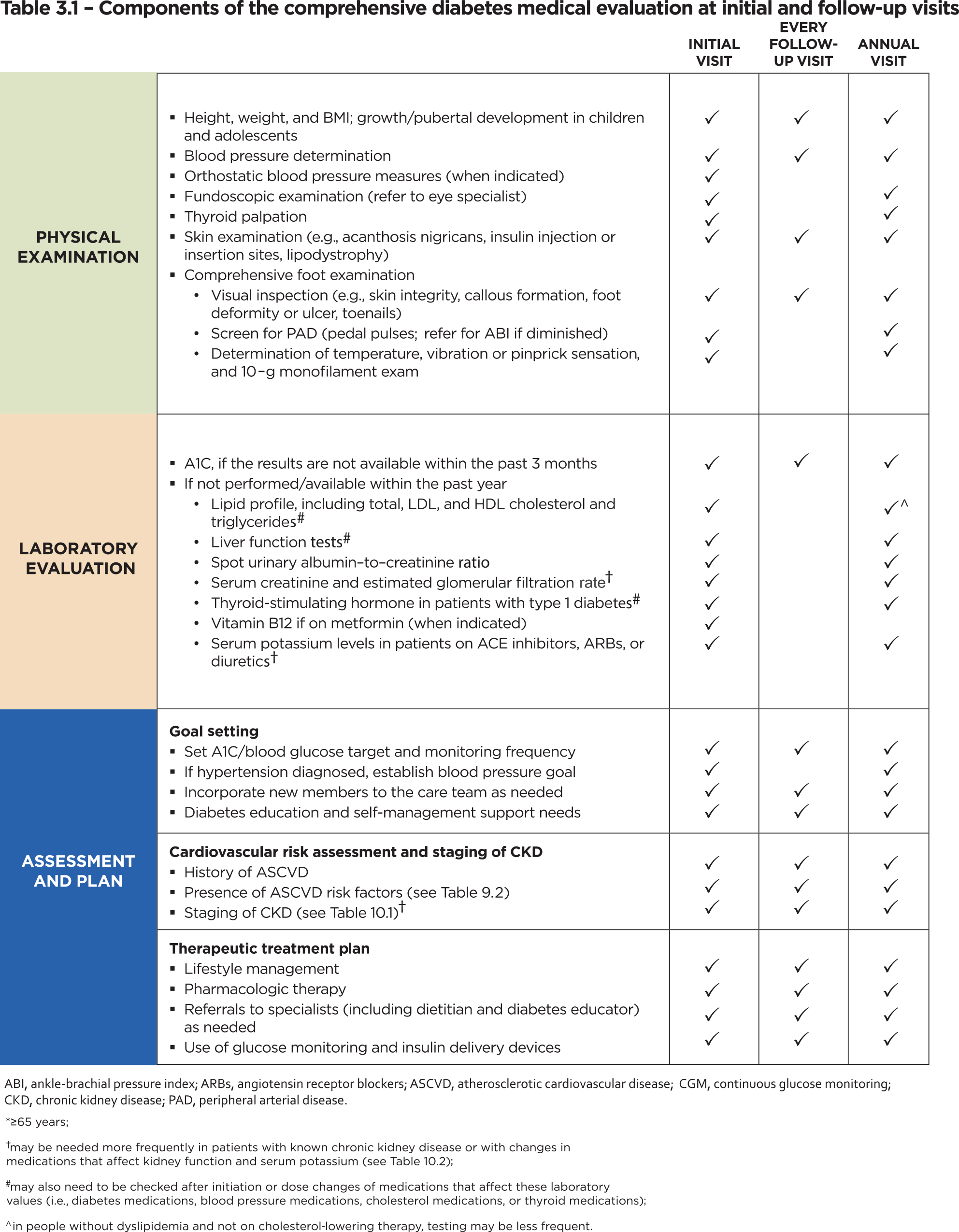
- A detailed table highlighting the components of a comprehensive medical evaluation has been redesigned and reorganized. It incorporates information about the recommended frequency of the components of care at both initial and follow-up visits, including regular screening for mental health. (Section 3, page S30, Table 3.1)
The Standards of Care are established and revised annually by the ADA's Professional Practice Committee (PPC). The committee is a multidisciplinary team of 12 leading U.S. experts in the field of diabetes care, and includes physicians, diabetes educators, registered dietitians and others whose experience includes adult and pediatric endocrinology, epidemiology, public health, lipid research, hypertension, preconception planning and pregnancy care. For the 2018 Standards of Care, two designated representatives from the American College of Cardiology reviewed and provided feedback for the PPC's recommendations for cardiovascular disease and risk management. Members of the committee must disclose potential conflicts of interest with industry and/or relevant organizations; these disclosures are available on page S154 of the 2018 Standards of Care. The complete supplement will be published online at http://care.diabetesjournals.org/content/41/Supplement_1 on December 8, 2017, as well as the Abridged 2018 Standards of Care.
About Diabetes Care®
Diabetes Care is a monthly journal of the American Diabetes Association dedicated to increasing knowledge, stimulating research and promoting better health care for people with diabetes. To achieve these goals, the journal publishes original articles on human studies in the following categories: clinical care, education and nutrition; epidemiology, health services; and psychosocial research; emerging treatments and technologies; and pathophysiology and complications. The journal also publishes the ADA's recommendations and statements, clinically relevant review articles, editorials and commentaries. Topics covered are of interest to clinically oriented physicians, researchers, epidemiologists, psychologists, diabetes educators and other health professionals. Diabetes Care is the highest-ranked, peer-reviewed journal in the field of diabetes treatment and prevention.
About the American Diabetes Association
Nearly half of American adults have diabetes or prediabetes; more than 30 million adults and children have diabetes; and every 21 seconds, another individual is diagnosed with diabetes in the U.S. Founded in 1940, the American Diabetes Association (ADA) is the nation's leading voluntary health organization whose mission is to prevent and cure diabetes, and to improve the lives of all people affected by diabetes. The ADA drives discovery by funding research to treat, manage and prevent all types of diabetes, as well as to search for cures; raises voice to the urgency of the diabetes epidemic; and works to safeguard policies and programs that protect people with diabetes. In addition, the ADA supports people living with diabetes, those at risk of developing diabetes, and the health care professionals who serve them through information and programs that can improve health outcomes and quality of life. For more information, please call the ADA at 1-800-DIABETES (1-800-342-2383) or visit diabetes.org. Information from both of these sources is available in English and Spanish. Find us on Facebook (American Diabetes Association), Twitter (@AmDiabetesAssn) and Instagram (@AmDiabetesAssn).
SOURCE American Diabetes Association







Share this article